Parapneumonic Pleural Effusion is Defined as Pleural Effusion Which Occurs in Association with Bacterial Pneumonia, Lung Abscess, or Bronchiectasis
General Comments
However, in Some Cases, an Infected Pleural Effusion May Rarely Develop without an Apparent Adjacent Pneumonia
Uncomplicated Parapneumonic Effusion
Uncomplicated Parapneumonic Effusion is Defined as a Free-Flowing Sterile Pleural Effusion
Occurs with Movement of Lung Interstitial Fluid and Neutrophils Across the Visceral Pleura into the Pleural Space
Exudate with pH >7.2
Complicated Parapneumonic Effusion
Complicated Parapneumonic is Defined as the Bacterial Invasion of the Pleural Space, Neutrophil Influx, and Pleural Space Acidosis (Due to Anaerobic Utilization of Glucose by Neutrophils and Bacteria)
Exudate with pH <7.2
There is a Higher Incidence of Complicated Parapneumonic Effusion in Human Immunodeficiency Virus (HIV)/Acquired Immune Deficiency Syndrome (AIDS) (see Human Immunodeficiency Virus)
Empyema
Various Definitions
Vianna Definition of Empyema (JAMA, 1971) [MEDLINE]
Positive Pleural Fluid Culture or Pleural White Blood Cell Count >15,000/mm3 and Pleural Total Protein >3.0 g/dL
Weese Definition of Empyema (Arch Intern Med, 1973) [MEDLINE]
Pleural White Blood Cell COunt >500/mm3, Pleural Total Protein >2.5 g/dL, or Pleural Specific Gravity >1.018
Modern Definition of Empyema
Presence of Pus in the Pleural Space and/or Positive Gram Stain of Pleural Fluid
Positive Pleural Fluid Cultures are Not Required for the Diagnosis of Empyema, Since Pleural Fluid Cultures May Be Negative for Multiple Reasons
Anaerobic Organisms are Difficult to Culture
Insensitivity of Bacterial Culture Methods
Pleural Fluid Sampling Often Occurs After a Patient Has Already Received Antibiotics
Pleural Fluid Sampling Errors May Occur Due to Loculations with Aspiration of a Sterile Fluid Pocket, Adjacent to an Infected Fluid Pocket
Epidemiology
Parapneumonic Effusion
Parapneumonic Effusion Occurs in Approximately 40% of Hospitalized Patients with Bacterial Pneumonia (Am J Med, 1980) [MEDLINE]
Inadvertent Placement of Nasogastric (NG) Tube Into Pleural Space with Enteral Tube Feeding Infusion (see Nasogastric/Orogastric Tube)
Rheumatoid Arthritis (RA) (see Rheumatoid Arthritis): likely has increased risk of empyema
Protective Effect of Inhaled Corticosteroids Against the Development of Parapneumonic Pleural Effusion (see Corticosteroids)
Clinical Efficacy
Spanish Study of the Effect of Prior Inhaled Corticosteroids (in Both Asthma and COPD) on the Risk of Developing Parapneumonic Effusion in Association with Pneumonia (Am J Respir Crit Care Med, 2013) [MEDLINE]
Prior Use of Inhaled Corticosteroids Decreased the Risk of Parapneumonic Effusion in Association with Pneumonia
Prior Use of Inhaled Corticosteroids was Associated with Higher Pleural pH, Higher Pleural Glucose, Lower Pleural Protein, and Lower Pleural LDH
Empyema
In the Modern Antibiotic Era Through the Early 1970’s, Incidence of Empyema Had Decreased to Approximately 2-3% of All Pneumonias (Arch Intern Med, 1973)[MEDLINE]
However, from 1995 to
Parapneumonic effusions and empyema. Proc Am Thorac Soc. 2006;3(1):75 [MEDLINE]
Empyema: an increasing concern in Canada. Can Respir J. 2008;15(2):85 [MEDLINE]
Emergence of parapneumonic empyema in the USA. Thorax. 2011;66(8):663 [MEDLINE]
Two Decades of Thoracic Empyema in Ontario, Canada. Chest. 2020;157(5):1114 [MEDLINE]
Parapneumonic Effusion Occurs in 40% of Bacterial Pneumonias Cases (Am J Med, 1980) [MEDLINE]
Pneumonia Accounts for 55% of Parapneumonic Effusion Cases
Presence of Pleural Effusion at Emergency Department Presentation with Pneumonia Predicts an Increasing Likelihood of Being Admitted, Longer Hospital Stay, and Increased 30-Day Mortality Rate (see Community-Acquired Pneumonia) (Chest, 2016) [MEDLINE]
Animal Studies Indicate that a Mixed Pleural Space Infection with Both Aerobes and Anerobes is More Likely to Produce an Empyema than Infection with a Single Organism (J Pediatr Surg, 1994) [MEDLINE]
Mixed Aerobic and Anaerobic Empyema was Found in 23% of Cases (Chest, 1993) [MEDLINE]: mixed microaerophilic or aerobic Streptococci with anaerobes are a common combination (as these are all components of normal oral flora)
For These Reasons, Isolation of an Aerobic Organism Alone Does Not Eliminate the Need to Cover for Unrecovered Anaerobic Organisms
Microbiology of Pleural Space Infection Appears to Be Changing (Respirology, 2011) [MEDLINE]
Different Organisms Predominate in Pediatric vs Adult Cases
Different Organisms Predominate in Community-Acquired vs Hospital-Acquired Cases
Pneumococcal Vaccination Has Altered Streptococcus Pneumoniae Serotypes in Empyema
Organisms
Anerobes: anaerobes are present in 36-76% of empyemas (Chest, 1993) [MEDLINE]
Tuberculous Empyema is a Rare Manifestation in which Tuberculous Infection Results in a Neutrophil-Predominant Empyema: in contrast, tuberculous pleurisy is a lymphocytic-predominant effusion which occurs due an immunologic response to tuberculous proteins
Physiology
Exudative Stage: rapid accumulation of sterile fluid (with low WBC, low LDH, normal glucose, normal pH) in pleural space (probably from interstitium in lung/possibly some originates from visceral pleural capillaries also)
Progression can be arrested at this stage if treated with antibiotics alone
Fibropurulent Stage: accumulation of neutrophils, bacteria, fibrin, and cellular debris in pleural space (with resultant decrease in pH and glucose/increase in LDH/formation of loculations in space)
Organization Stage: fibroblasts grow into exudate from visceral and parietal pleura, creating an inelastic pleural peel
Thick exudate may drain through the chest wall (empyema necessitatis) or into the lung (bronchopleural fistula)
Indications for Thoracentesis in the Setting of Parapneumonic Effusion (Chest, 2000) [MEDLINE]
Free-Flowing Pleural Fluid Which Layers >25 mm on a Lateral Decubitus Chest X-Ray or Chest CT
Pleural Fluid Loculations
Thickened Parietal Pleural on Intravenous Contrast-Enhanced Chest CT: this is suggestive of empyema
Technique
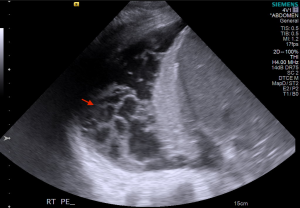
Ultrasound Guidance is Standard
Appearance
Example: empyema (purulent drainage) in pleurevac container
Odor
Foul-Smelling Odor: indicates the presence of anaerobic infection
Pleural Fluid Cell Count and Differential
xxx
Pleural Fluid pH
Decreased: pleural fluid pH >7.20 is considered the recommended threshold for pleural chest tube drainage (Chest, 2000) [MEDLINE]
Pleural Fluid pH is the Most Sensitive Indicator for Pleural Chest Tube Drainage (Am J Respir Crit Care Med, 1995) [MEDLINE]
Technique
Improper Processing of Pleural Fluid pH Samples Occurs in 30-50% of Labs in the US (Curr Opin Pulm Med, 2013) [MEDLINE]
Potential Errors in pH Measurement in Pleural Fluid Samples: exposure of sample to air, delay in measurement, use of pH meter instead of a blood gas machine
Decreased: pleural fluid glucose <60 mg/dL is considered the threshold for pleural chest tube drainage
Diagnostic Accuracy of Pleural Fluid Glucose for Parapneumonic Effusion is Less Sensitive than Pleural Fluid pH (Am J Respir Crit Care Med, 1995) [MEDLINE]: however, it may be useful when pleural fluid pH is not available
Pleural Fluid Total Protein
Pleural Fluid Total Protein/Serum Total Protein Ratio >0.5
Pleural Fluid LDH is Increased Due to the Lysis of Neutrophils
Pleural Fluid LDH >66% of Upper Limit of Normal Range for Serum LDH
Pleural Fluid LDH May Be >1000 IU/L in Some Cases
Serum-Pleural Albumin Gradient (SPAG)
Serum-Pleural Albumin Gradient (SPAG) <1.2 g/dl
If Fluid Clinically Appears to be a Transudate and SPAG >1.2, but Light’s Criteria Suggest Exudate, Pleural Fluid Can Be Assumed to Be a Transudate: due to the fact that albumin is lower molecular weight than other proteins and crosses capillary walls more easily
Acid-Fast Bacteria (AFB) Stain: useful to identify etiologic organism
Pleural Fluid Culture
Sensitivity of Pleural Fluid CUlture
Pleural Fluid Culture is Often Negative in Empyema: since animal models demonstrate that bacteria are typically cleared rapidly from the pleural space (Ann Thoracic Surg, 1987) [MEDLINE]
Anerobic Organisms are Difficult to Isolate by Pleural Fluid (and Blood) Culture: increased sensitivity for detection of anaerobes may be provided by molecular methods (Chest, 2011) [MEDLINE]
Use of Blood Culture Bottles to Culture Pleural Fluid: use of blood culture bottles (in addition to standard culture) improves the sensitivity of pleural fluid culture (Thorax, 2011) [MEDLINE]
Molecular Analysis of Pleural Fluid
PCR or Rapid Antigen Assay for Streptococcus Pneumioniae: these increase sensitivity for detection of Streptococcus Pneumioniae (Clin Infect Dis, 2006) [MEDLINE]
Quantification of Pleural Fluid: using upright and lateral decubitus chest x-ray to determine the extent of layering
Detection of Pleural Fluid Loculation: may be seen on chest x-ray in some cases
Recommendations (American Association for Thoracic Surgery Emypema Guidelines 2017) (J Thorac Cardiovasc Surg, 2017)[MEDLINE]
Presence of a Pleural Effusion Should Be Investigated in All Patients with Symptoms of Pneumonia or Unexplained Sepsis (Class: 1, LOE: B)
Pleural Fluid Analysis is Mandatory Since Patients with Complicated Parapneumonic Effusions Do Not Clinically Differ from Patients with Simple Effusions on the Basis of Clinical Presentation Alone
Failure of a Community-or Healthcare-Associated Pneumonia to Clinically Respond to Appropriate Antibiotic Therapy Should Prompt Investigations to Identify the Presence of a Pleural Effusion (Class: 1, LOE: B)
Intravenous Contrast Accentuates the Pleural Line: this aids in the differentiation of parenchymal consolidation vs a pleural collection
Indications
Quantification of Pleural Fluid
Identification of Endobronchial Lesions
Identification of Associated Pneumonia/Lung Abscess (see Pneumonia and Lung Abscess)
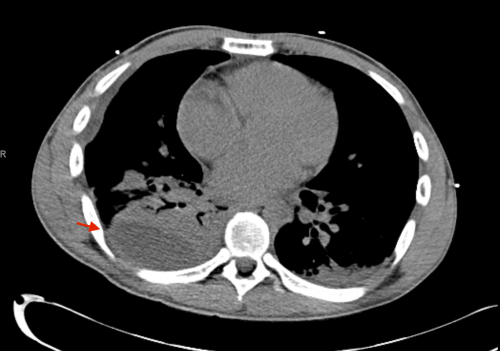
Detection of Pleural Fluid Loculation and Localization for Potential CT-Guided Chest Tube Placement
Example: red arrow indicates loculated posterior pleural effusion which was amenable to single CT-guided chest tube drainage
Findings
Gas Microbubbles within the Pleural Space
Pleural Space Gas Microbubbles on Chest CT Occurred in 58% of Empyema Cases (Clin Radiol, 2006) [MEDLINE]
Pleural Space Gas Microbubbles Predicted an Increased Need for Repeated Drainage (65.9% vs 36.7%; p=0.015) and Surgical Decortication (31.7% vs 6.7%; p=0.011) (Clin Radiol, 2006) [MEDLINE]
Pleural Space Gas Microbubbles Did Not Impact the Mortality Rate (9.8% vs 6.6%; p=0.53) (Clin Radiol, 2006) [MEDLINE]
“Split Pleura Sign” (with Chest CT with Intravenous Contrast): thickening of the visceral and parietal pleura with >30 mm of separation of the pleural surfaces
Pleural Fluid Loculation
Pleural Fluid Microbubbles: presence of microbubbles within the pleural fluid collection (which presumably are introduced via a prior thoracentesis) suggest that the fluid will be more resistant to chest tube drainage (Clin Radiol, 2006) [MEDLINE]
Chest Computed Tomography (Chest CT) Findings Which Allow Differentiation of Empyema from Lung Abscess (see Lung Abscess)
Chest Computed Tomography (Chest CT) Features Suggestive of Empyema
Air-Fluid Level: may be seen in cases with an associated bronchopleural fistula (see Bronchopleural Fistula)
Angles: “ball under the carpet” appearance (obtuse angles between fluid collection and chest wall)
Displacement: displacement of lung and mediastinum, as empyema pushes adjacent structures toward contralateral side
Internal Surface: typically smooth internal surface of fluid collection
Shape: lenticular shape
“Split Pleura Sign”: separation of parietal and visceral pleura
Chest Computed Tomography (Chest CT) Features Suggestive of Lung Abscess (see Lung Abscess)
Air-Fluid Level: may be seen
Angles: acute angles between fluid collection and chest wall
Displacement: lack of displacement of lung and mediastinum, as abscess tends to destroy adjacent lung, rather than displace it
Internal Surface: typically thick, irregular internal surface of fluid collection
Shape: typically round shape
Recommendations (American Association for Thoracic Surgery Emypema Guidelines 2017) (J Thorac Cardiovasc Surg, 2017)[MEDLINE]
Higher VEGF Level or Larger Effusion was Associated with Decreased Fibrinolytic Activity, Development of Pleural Fluid Loculation and Fibrosis, and Higher Risk of Medical Treatment Failure
ACCP Consensus Guidelines Classification of Parapneumonic Effusion (Chest, 2000) [MEDLINE]
Category 1: very low risk of poor outcome -> drainage not recommended
Minimal Free Flowing and <10 mm on Lateral Decubitus CXR: A0
Pleural Fluid Gram Stain and Culture Results Unknown: Bx
Pleural Fluid pH Unknown: Cx
Category 2: low risk of poor outcome -> drainage not recommended
Small-Moderate Free Flowing and <10 mm on Lateral Decubitus CXR and Less than 50% of the Hemithorax: A1
Negative Pleural Fluid Gram Stain and Culture: B0
Pleural Fluid pH ≥7.20: C0
Category 3: moderate risk of poor outcome -> drainage recommended
Large Free Flowing (≥50% of Hemithorax), Loculated Effusion, or Effusion with Thickened Parietal Pleura: A2
Positive Pleural Fluid Gram Stain or Culture: B1
Pleural Fluid pH <7.20
Category 4: high risk of poor outcome -> drainage recommended
Large Free Flowing (≥50% of Hemithorax), Loculated Effusion, or Effusion with Thickened Parietal Pleura: A2
Pus: B2
Pleural Fluid pH <7.20
Clinical Manifestations
General Comments
Time Course of Presentation
Time Course of Parapneumonic Effusion Depends on the Underlying Organism, Host Immunocompetence, and Timing of the Patient’s Presentation for Medical Care
Anerobic Emypema: may present after a longer time course (may be as long as weeks in duration)
Average Duration of Symptoms in Patients with Empyema Prior to Presentation is Approximately 2 wks (NEJM, 2005) [MEDLINE]
Increased RAPID Score Predicted Mortality and Increased Hospital Length of Stay
Study of RAPID Score to Predict Long-Term Outcome in Pleural Space Infection at Presentation for Pneumonia (Ann Am Thorac Soc, 2015)
Increased RAPID Score Predicted Mortality Rate at 3 mo and 1/3/5 yrs
Factors Associated with High-Risk RAPID Scores: Gram-negative rod infections, heart disease, diabetes mellitus, lung disease, and increased length of stay
German Study of the Adjustment of the RAPID Score with 2 Additional Variables (Sci Rep, 2023) [MEDLINE]
Diabetes type 1 and 2, renal replacement therapy, immunosuppression, postoperative bleeding, intraoperative transfusion as well as microbiologically confirmed bacterial invasion of the pleura all led to higher mortality rates
Modifying the RAPID Score by Adding the Comorbidities Diabetes Mellitus and Need for Renal Replacement Therapy Significantly Increased the Predictive Value of the RAPID Score
Prepare (in Sterile Manner) 10 mg in 25 mL of Normal Saline in a 60 mL Catheter-Tip Syringe
With Two Chest Tube Clamps in Place, Unclamp Chest Tube and Instill Alteplase
Flush with Sterile 25 ml Saline in 60 mL Catheter-Tip Syringe
Clamp Chest Tube for 2 hrs, Then Place Chest Tube Back to Suction
Administer 10 mg in normal saline BID x 3 days
Injection via silastic self-sealing (pleurevac) tubing with 20 gauge needle
Clinical Efficacy
First Multicenter Intrapleural Sepsis Trial (MIST1) (NEJM, 2005) [MEDLINE]
Intrapleural Streptokinase Did Not Improve Mortality, Rate of Surgery, or Length of Hospital Stay in Patients with Pleural Space Infection
MIST2 Trial Comparing Intrapleural Tissue Plasminogen Activator with/without DNase in Pleural Space Infection (NEJM, 2011) [MEDLINE]: n = 210 patients (blinded 2 x 2 factorial trial)
Intrapleural tPA + DNase Therapy Improved Drainage, Decreased the Frequency of Surgical Referral, and Decreased the Duration of Hospital Stay
Treatment with Either tPA + DNase Alone Had No Clinical Benefit
DNase Treatment Alone Resulted in a 3x Increase in the Number of Surgical Referrals Due to Worsening Infection
Association between intrapleural urokinase monotherapy and treatment failure in patients with pleural infection: a retrospective cohort study. BMC Pulm Med. 2023;23(1):273. doi:10.1186/s12890-023-02559-5 [MEDLINE]
Background: Pleural infection, an infection of the pleural space, is frequently treated with antibiotics and thoracic tube drainage. In case of insufficient drainage, an intrapleural fibrinolytic agent is considered before surgical intervention. However, the effectiveness of fibrinolytic monotherapy is still controversial. Therefore, we aimed to examine the association between urokinase monotherapy and treatment failure in patients with pleural infection
Methods: In this retrospective observational study, patients with pleural infection underwent chest tube insertion were divided into two groups including patients treated with or without intrapleural instillation of urokinase. The propensity score overlap weighting was used to balance the baseline characteristics between the groups. Treatment failure was defined by the composite primary outcome of in-hospital death and referral for surgery
Results: Among the 94 patients, 67 and 27 patients were in the urokinase and non-urokinase groups, respectively. Urokinase monotherapy improved the composite outcome between the groups (19.4% vs. 48.1%, p = 0.01). After adjusting using propensity score overlap weighting, urokinase monotherapy improved the composite outcome compared to the non-urokinase group (19.0% vs. 59.5%, p = 0.003)
Conclusions: Urokinase monotherapy can be an important nonsurgical treatment option for patients with pleural infection.
Pleural Space Drainage: VATS pleural drainage is the standard treatment for patients who fail chest tube drainage
Conversion Rate to Thoracotomy: 3% (Ann Thorac Surg, 2006) [MEDLINE]
Pleural Decortication (see Pleural Decortication): considered when symptomatic restriction of lung expansion (due to fibrothorax) is still present >6 mo after initial event
Prognosis
Study of Impact of Parapneumonic Effusion Associated with Pneumonia at Hospital Admission on Outcome (Chest, 2016) [MEDLINE]
Presence of Pleural Effusion at Emergency Department Presentation with Pneumonia Predicts an Increasing Likelihood of Being Admitted, Longer Hospital Stay, and Increased 30-Day Mortality Rate
References
General
Nontuberculous bacterial empyema in patients with and without underlying diseases. JAMA. 1971 Jan 4;215(1):69-75 [MEDLINE]
Empyema of the thorax then and now. A study of 122 cases over four decades. Arch Intern Med. 1973 Apr;131(4):516-20 [MEDLINE]
Parapneumonic effusions. Am J Med. 1980;69(4):507 [MEDLINE]
Experimental aerobic-anaerobic thoracic empyema in the guinea pig. Ann Thorac Surg. 1987;43(3):298 [MEDLINE]
Aerobic and anaerobic microbiology of empyema. A retrospective review in two military hospitals. Chest. 1993;103(5):1502 [MEDLINE]
A bacteriologic basis for the evolution and severity of empyema. J Pediatr Surg. 1994;29(5):667 [MEDLINE]
Pleural fluid chemical analysis in parapneumonic effusions. A meta-analysis. Am J Respir Crit Care Med. 1995;151(6):1700 [MEDLINE]
Microbiological diagnosis of empyema in children: comparative evaluations by culture, polymerase chain reaction, and pneumococcal antigen detection in pleural fluids. Clin Infect Dis. 2006;42(8):1135 [MEDLINE]
Prevalence and clinical significance of pleural microbubbles in computed tomography of thoracic empyema. Clin Radiol. 2006;61(6):513 [MEDLINE]
Predominant role of bacterial pneumonia as a cause of death in pandemic influenza: implications for pandemic influenza preparedness. J Infect Dis. 2008;198(7):962 [MEDLINE]
Blood culture bottle culture of pleural fluid in pleural infection. Thorax. 2011;66(8):658 [MEDLINE]
A higher significance of anaerobes: the clone library analysis of bacterial pleurisy. Chest. 2011;139(3):600 [MEDLINE]
Pleural infection: changing bacteriology and its implications. Respirology. 2011 May;16(4):598-603 [MEDLINE]
Influence of previous use of inhaled corticoids on the development of pleural effusion in community-acquired pneumonia. Am J Respir Crit Care Med. 2013;187(11):1241 [MEDLINE]
Clinical importance of angiogenic cytokines, fibrinolytic activity and effusion size in parapneumonic effusions. PLoS One. 2013;8(1):e53169. Epub 2013 Jan 7 [MEDLINE]
Procalcitonin as a diagnostic marker in differentiating parapneumonic effusion from tuberculous pleurisy or malignant effusion. Clin Biochem. 2013;46(15):1484 [MEDLINE]
Do we measure pleural fluid pH correctly? Curr Opin Pulm Med. 2013 Jul;19(4):357-61 [MEDLINE]
A clinical score (RAPID) to identify those at risk for poor outcome at presentation in patients with pleural infection. Chest. 2014 Apr;145(4):848-55 [MEDLINE]
Predicting Long-Term Outcomes in Pleural Infections. RAPID Score for Risk Stratification. Ann Am Thorac Soc. 2015 Sep;12(9):1310-6 [MEDLINE]
Pleural Effusions at First ED Encounter Predict Worse Clinical Outcomes in Patients With Pneumonia. Chest. 2016;149(6):1509 [MEDLINE]
Treatment
Medical and surgical treatment of parapneumonic effusions : an evidence-based guideline. Chest. 2000 Oct;118(4):1158-71 [MEDLINE]
MIST1 Trial. U.K. Controlled trial of intrapleural streptokinase for pleural infection. N Engl J Med. 2005 Mar 3;352(9):865-74 [MEDLINE]
Video-assisted thoracic surgery for pleural empyema. Ann Thorac Surg. 2006;81(1):309 [MEDLINE]
Intrapleural administration of Pulmozyme for pleural empyema. Respiratory Medicine CME 2011, Vol.4(3):114–115, doi:10.1016/j.rmedc.2010.12.002
MIST2 Trial. Intrapleural Use of Tissue Plasminogen Activator and DNase in Pleural Infection. N Engl J Med. 2011 Aug 11;365(6):518-26. doi: 10.1056/NEJMoa1012740 [MEDLINE]
Is medical thoracoscopy efficient in the management of multiloculated and organized thoracic empyema? Respiration. 2012;84(3):219 [MEDLINE]
Intrapleural tissue plasminogen activator and deoxyribonuclease therapy for pleural infection. J Thorac Dis. 2015 Jun;7(6):999-1008 [MEDLINE]
New therapy of pleural empyema by deoxyribonuclease. Braz J Infect Dis. 2013 Jan-Feb;17(1):90-3. doi: 10.1016/j.bjid.2012.08.019. Epub 2013 Jan 16 [MEDLINE]